Whitepaper
Pre-Licensed Therapists: The Missing Link in the Behavioral Health Workforce Shortage

Executive Summary
Collaborative care, whole-person care, value-based care…
The future of healthcare involves integrating behavioral healthcare into patient care.
But when the daily realities of the behavioral health workforce crisis are burgeoning waitlists, emergency care, and unanswered job postings — it’s hard to get past today.
How do you reshape care delivery when there is no one to deliver care to the patient?
And how do you meet HEDIS measures, contract obligations, and new state initiatives demanding rapid access to behavioral health care?
Every year, 48,000 new clinicians graduate from Master’s level programs with extensive training and hundreds of hours of direct clinical experience. They start the long journey to accumulate 3,000+ clinical hours under clinical supervision before they can take their licensure exam, usually 2-3 years later.
57% will leave the field in their first 2-3 years — one of the biggest reasons is difficulty finding work in their field. Most behavioral healthcare providers specify “licensed therapists” when advertising open positions.
It is time to reconsider whether pre-licensed therapists can provide the level of quality care that will meet the drastic need our nation is experiencing and also consider what other benefits early-career clinicians can bring to organizations and the patients they serve.
Table of Contents
What is the best clinical supervision option?

Feeling the Behavioral Health Workforce Shortage
For the 2nd year in a row, the American College of Healthcare Executives Survey reports that workforce challenges top their list of concerns. Nearly all the top-reported concerns were connected to patient care.
While this survey captures trends in healthcare as a whole, behavioral health executives echo the same concerns.
A drastic therapist shortage causes the other listed concerns to topple like dominoes. How can employers improve access, fulfill contracts and mandates, and ensure patient care, quality, and safety if no one is available to provide the actual care?
Substantive changes that would drive access and improve affordability can’t happen if there aren’t enough behavioral health professionals in the workforce.
Workforce challenges, especially personnel shortages and burnout
Behavioral health and addiction issues, particularly the lack of available resources in the community
Access to care
Government mandates
Patient safety and quality of care — meeting HEDIS and CMS Universal Foundation Quality Measures (1)
How the worker shortage is affecting those who need help
50% of the U.S. population lives in mental health shortage areas (also known as HPSAs). The shortage severely impacts rural and urban communities alike. (2)
56% of psychologists say they have no openings and their average waitlists are over three months. 40% say their waitlists have grown in the last year. (3)
55% of adults and 84% of children and adolescents will be discharged without seeing a mental health professional (4)
In 2020, 53% of adults with a history of serious mental illness reported that they did not receive help when they needed it over the past year. (5)
Behavioral health employers know what these statistics look like in real life: waitlists, constant clinician turnover, burnout, and an inability to move forward in any positive direction.
Pre-licensed therapists have graduated from a Master’s program including clinical internship/practicum. They have not qualified for their license to practice independently.
Before they sit for their examination, they will accumulate 2,000 – 4,000 clinical hours under a clinical supervisor. This process takes a minimum of two years.
Pre-licensed clinicians are fully qualified to conduct therapy with patients.
The answer that should be obvious, but isn’t
Our best hope for solving the worker shortage is the 48,000 clinicians who graduate every year, but graduation is where they enter the most arduous part of their journey.
Once they graduate with their Master’s degrees, they will need to secure positions that will allow them to accumulate 2,000 – 4,000 hours of clinical experience before they can take their examination and qualify for their licenses to practice independently.
LinkedIn and Indeed job listings reflect the worker shortage. Open positions abound.
Almost all of them specify “license required.”
Of the 48,000 who graduate every year, 57% will leave the counseling profession within the first 2 -3 years — the most common reason given is they can’t find work that will cover their expenses. (6)
Behavioral health employers are struggling to fill positions, patients are languishing on ever-expanding waiting lists, and 27,000 pre-licensed clinicians can’t find work.
This shouldn’t be happening.
That’s nearly 80,000 therapists from the last three years that experienced financial, academic, experience, supervision, or regulatory barriers that kept them from moving forward.
Reasons for not obtaining licensure:
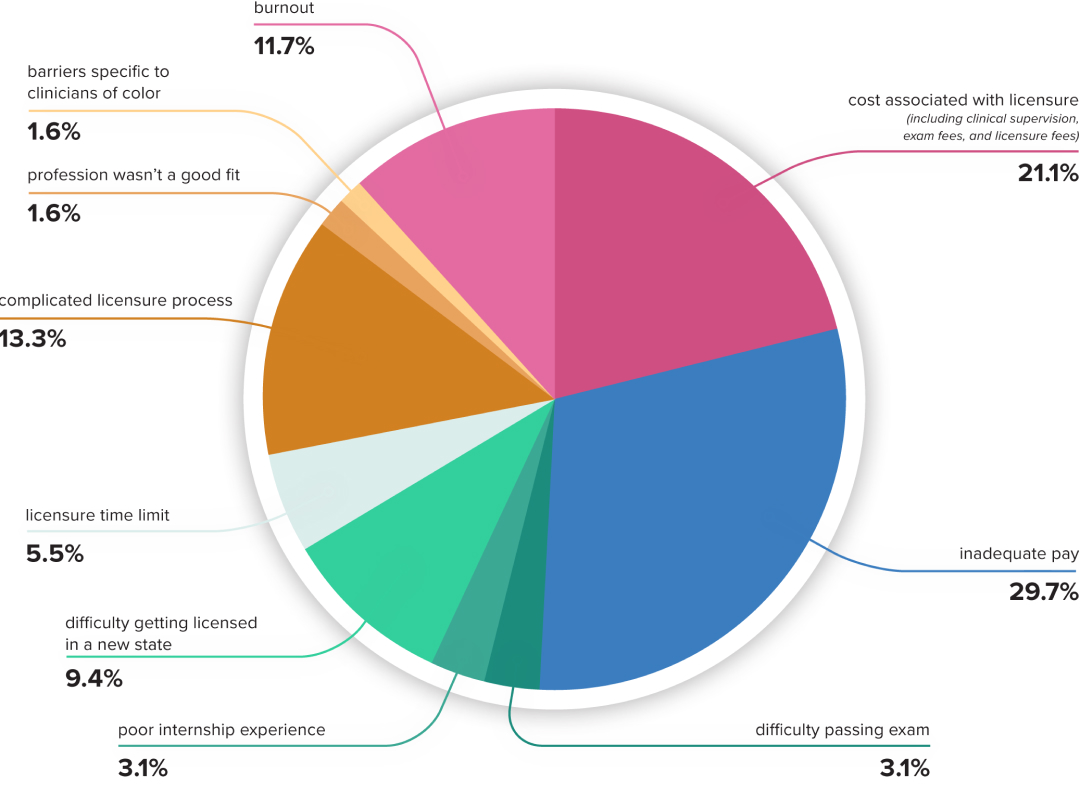
Tap image to enlarge
4 reasons why employers avoid working with pre-licensed counselors
Mainstream behavioral health employers hesitate to employ pre-licensed counselors for four reasons:
1.
Fear that quality care may be compromised
“Health plans are prioritizing quality, access, and affordability,” according to Briana Duffy, President of External Markets at Carelon Health. (7)
The importance of quality of care cannot be understated. Inadequate care is costly: ineffective therapy causes harm to the patient and wastes financial resources.
The pandemic shutdown demonstrated how physical and mental healthcare intertwine like a Gordian knot. They can’t be separated from each other. In the first few months of the shutdown, depression, anxiety, and substance use disorders catapulted the onset of chronic and dangerous health conditions.
Health plans and provider companies are motivated to prioritize mental healthcare, but they need to invest with purpose and test for effectiveness.
Responsible testing means controlling variables that could muddle the data.
If experience correlates positively with quality care, then inexperienced clinicians are a potential confounding variable. Insisting on licensed therapists evens the playing field and guarantees experience.
But have they tested whether experience correlates positively with quality care?
2.
Potential expense and infrastructure costs to ensure compliance with state regulations
Many employers believe that pre-licensed clinicians bring unnecessary and potentially expensive complications. If therapists aren’t licensed, state regulations require them to meet regularly with a clinical supervisor.
Community-based care, state and local agencies, and federal programs like the Veterans Administration are among those willing to employ pre-licensed clinicians. If they’re providing clinical supervision for their therapists, they typically choose one of these options:
Supervision option
Employ a clinical director
Benefits
- Supervision is part of their job description.
- Regular awareness of the supervisee’s performance.
- Ability to combine organizational training with clinical training.
Downsides
- If a supervisor leaves, the supervisee may not be able to meet with patients. Patients do not receive care
- Supervisors with a broad range of responsibilities may not be able to focus on their supervisees and give them the support they need.
- Fully licensed therapists often prefer to work in private practice rather than in the community-based setting.
Supervision option
Assign supervision duties to other licensed clinical staff members
Benefits
- As employees, they know the population the organization serves.
Downsides
- Clinical supervision has different goals and processes than therapy, amplifying a therapist’s workload.
- Time may be better devoted to patient care.
- Sometimes, the supervisee is a peer or direct report of the supervisor, either of which complicates the professional relationship.
Supervision option
Contract a clinical supervisor from an outside organization
Benefits
- Alleviates pressure on in-house staff to fulfill this role.
- Only paying for supervision and administration hours. It’s cost-effective for some situations.
- Gives supervisees an additional perspective.
Downsides
- Can be difficult to find, especially in shortage areas.
- Difficult to track progress and compliance if communication is difficult.
- If clinical supervisors let their qualifications lapse, it can jeopardize patient care and boards may not count supervision or clinical hours.
3.
Lack of awareness about the unique licensure process for behavioral health clinicians
The behavioral health licensure process differs from that of other professions. Attorneys, accountants, teachers, and most medical professionals take their respective exams shortly after graduation, and physicians take the USMLE as part of their program.
Depending on the state and license, the licensure process for behavioral health professionals takes a minimum of 2-4 years to complete after clinicians earn their Master’s degrees.
Requirement
Master’s degree practicum & internship
Length of time to fulfill
Approximately 2-3 years
150 face-to-face hours (varies by state) – 300 for total clinical practicum and internship.
Requirement
Pre-licensure period (associate clinician)
Length of time to fulfill
2,000 – 4,000 hours depending on the state (3,000 is the average). 2-3 years of direct client work or longer. Most states specify no less than 2 years.
Requirement
Licensure exam
Length of time to fulfill
Clinicians must pass the licensure exam before applying for state licensure.
4.
Concern that they can’t get reimbursed for the care they provide
Historically, only Medicaid serving organizations employed pre-licensed clinicians because those were the only organizations who could get reimbursed for their care. That left a huge gap for commercially serving organizations who struggled to find licensed clinicians.
However, things have changed in the recent years. Many commercial insurance companies now allow for pre-licensed clinicians to see patients while under supervision and bill under their supervisor’s NPI.
Many employers don’t know this option exists.
What is a clinical supervisor?
A clinical supervisor is a licensed therapist who has met state requirements to provide mentorship and guidance to pre-licensed therapists.
During the years of clinical supervision, the supervisor will lead them through refining their clinical skills, review their cases regularly, help them navigate ethical situations, and act as a “gatekeeper” of the profession — mentoring them while also assessing their competency.
When clinical supervision approaches completion, the clinical supervisor provides documentation and attests to the supervisee’s professional capabilities.
The Long Walk to Licensure
Legislators, policymakers, and other professionals outside of the mental health world often have little understanding of the costs and challenges associated with mental health licensure. They may not know that it typically takes a minimum of two years of full-time supervised practice to be eligible for independent licensure as a clinician.
Many outside the field focus advocacy efforts on scholarship and loan reimbursement programs, figuring that it is a short walk from the degree to licensure.
But part of the reason these programs have little impact is that it’s actually quite a long walk from graduation to licensure, much more so than for most other professions — including health care professions.

Ben Caldwell, Psy.D.
Founder, High Pass Education

The Big Question: Do pre-licensed clinicians deliver lower-quality care?
Patients rely on their therapists to support them and provide them with the tools to heal from whatever struggles they are facing. Any problem important enough to bring a patient into therapy deserves serious attention — but sometimes, these problems are debilitating or even life-threatening.
Cost-effectiveness is also an issue for organizations, health plans, and providers. When a patient receives adequate care, they proceed through the treatment process quickly and make room for the next patient.
Many employers consider a licensed therapist to be a safer choice.
Pre-licensed doesn’t mean inexperienced
As part of an accredited degree program, therapy students gain experience working with patients in clinical situations under the supervision of a licensed clinician, either at a program-run clinic or at an organization approved by their school.
During this practicum and internship, they engage in face-to-face counseling in different settings (individual, couples, family, adolescent, etc.) while receiving feedback and guidance from their site supervisor.
By the time they don their caps and gowns, pre-licensed clinicians have faced challenging situations and supported several clients through crisis and mental illness.
Pre-licensed clinicians are already proving themselves in challenging situations
Many of the organizations, agencies, and behavioral health hospitals that employ pre-licensed clinicians serve challenging and complicated populations.
Pre-licensed clinicians working in these venues counsel patients experiencing co-occurring disorders, trauma, schizophrenia, and other challenging diagnoses. Their patients may be involved with child protective services or prison systems or have inadequate food, shelter, or income.
The employers who regularly work with pre-licensed counselors trust them to navigate difficult and complex situations.
Does the quality of care correlate with clinical experience?
A considerable amount of published research engages the question, “Do experienced counselors deliver better care?” The chart below focuses on larger studies that compared clinicians with varying levels of experience:
Study
Description
A literature review comparing therapist experience and patients with major depressive disorder or anxiety disorders (internalizing disorders).
Results
Experience positively correlated with length of treatment for patients with major depressive disorder.
No noticeable difference between therapists with less or more experience when treating anxiety disorders.
Any difference disappeared with the inclusion of clinical supervision or manualized treatment. (8)
Study
Erekson, et al., (2017)
Description
Studied student psychologists in various stages of their training. Administered Outcome Questionaire-45 (OQ-45) to patients after each session.
Results
Therapists in later stages effected slower rates of change in their patients than at earlier stages of training. (9)
Study
Chow, et al., (2015)
Description
Studied the relationship between client outcome and therapist demographics, professional development activities, and their work practices.
Results
“years of experience, gender, age, profession, highest qualification, caseload, and degree of theoretical integration did not significantly predict client-reported outcomes. Consistent with the literature on expertise and expert performance, the amount of time spent targeted at improving therapeutic skills was a significant predictor of client outcomes.” (10)
Study
Budge, et al., (2013)
Description
Studied psychotherapists at different experience levels — beginning practicum, advanced practicum, internship/postdoctorate, and licensed psychologist.
Results
Therapists in the internship/postdoctorate phase (receiving clinical supervision) effected more change and symptom reduction than both practicum students and licensed psychologists. (11)
Study
Goldberg, et al., (2016)
Description
A longitudinal study examining efficacy and increased experience over time.
Results
As a whole, therapists became slightly less effective over time with 60.59% diminishing in skill and 39.41% showing improvement. The magnitude was extremely small but remained statistically significant despite adjustments. (12)
The research doesn’t support the conclusion that licensure guarantees clinical quality…
The biggest indicator of quality care for clinicians of all levels of experience is a consistent commitment to improving their clinical skills. This positively correlates with greater change in their patients.
In the studies above, the therapists who exhibited the most success with their patients were in their prelicensure period under the guidance of their clinical supervisors.
The prelicensure period is one of the most effective stages of a clinician’s entire career. These years are specifically devoted to building experience and refining the clinician’s therapeutic skills.
Does the quality of care correlate with clinical experience?
1
Pre-licensed clinicians bring energy and devotion to their work and organizations. They’ve committed so much of their energy and resources to this work. They form therapeutic bonds easily and those bonds cause meaningful change in the patients. (13)
2
Pre-licensed clinicians are not on their own. Employers get the benefits of working with a newer clinician as well as the experience and guidance of the clinical supervisor. Whether the clinical supervisor works for the same organization or not, a major aspect of the supervisor’s responsibility is to safeguard the patient’s welfare and ensure the clinician is providing quality care. (14)
3
Pre-licensed clinicians have had access to the latest research and evidence-based approaches. As recent graduates, the latest clinical models might be more top-of-mind for new clinicians than for a clinician who has been practicing for several years.
4
Pre-licensed clinicians are malleable. As health plans are implementing technological, value-based, or integrated care solutions, pre-licensed clinicians are open to new approaches in treatment management and are more willing to take direction. (15)
Pre-licensed clinicians alleviate recruitment and retention challenges
When employers provide clinical supervision as a benefit, it’s a huge incentive for the pre-licensed applicant to accept the position.
The current turnover rate for behavioral health positions is 30-60% annually. (16)
This revolving-door cycle of recruitment/resignation threatens quality and consistency of care for patients and demoralizes staff members. If the clinician is receiving quality clinical supervision, they have an incentive to stay for at least 2-3 years. That’s double the current average retention rate.
If the workplace prioritizes respect, adequate pay, and potential for growth, therapists have more reason to continue with an employer even after they earn their licenses to practice independently.

What is the best clinical supervision option?
Working with pre-licensed clinicians opens up possibilities for organizations that need to fill positions, improve access for their patients, and even expand staff diversity so their patients have more care options.
As part of the decision-making process, employers must decide which clinical supervision solution is best for their organization. If they operate in multiple states or employ therapists under multiple licenses, the best solution may differ in each state.
What to consider when deciding on clinical supervision
Employers have three basic options. The first two, in-house supervision or external clinical supervision with an onsite, contracted clinical supervisor, have been around for a long time. But since the pandemic shutdown, a new option has emerged — virtual clinical supervision.
Many organizations choose to handle clinical supervision in-house, but they should evaluate whether they have the resources to do so:
1
Is there a clinical director or supervisor on staff who can take on these responsibilities or do they have the means and willingness to bring one on staff?
2
Are there licensed staff members who are willing to add clinical supervision responsibilities to their caseloads?
3
Would it benefit the organization more if the time required for staff to conduct clinical supervision was devoted to other administrative projects or tasks… or to patient care? Employers should consider the potential for burnout as they evaluate this.
4
Is there a safety net if the person fulfilling the clinical supervisor role leaves the organization — or would patient care need to stop until a replacement is found?
If qualified clinicians are willing to take up the task without risking burnout, then handling clinical supervision in-house might be a good option – but it might not be the right answer for every facility operating under the same umbrella.
Some behavioral health professionals offer individual and/or group clinical supervision for a fee. This can be an advantage, especially for a smaller organization with fewer pre-licensed clinicians.
Some aspects to consider when searching for the right clinical supervisor:
1
Can they provide proof they’re qualified to offer clinical supervision in that state for the licenses the pre-licensed counselors are pursuing?
2
Can they provide documentation that they’re not currently under any kind of discipline with their state board?
3
Have they worked with your patient population or in a similar environment so they can provide insights that will help the supervisees as they work with their caseloads?
4
How will the employer and clinical supervisor handle communication and supervision updates?
5
How is necessary documentation managed?
6
Will the supervisor have access to the EHR to gain insight into their supervisee’s caseload?
7
Does the supervisor track state regulation changes so clinical supervision remains compliant? If changes are missed, the supervisee’s clinical and supervision hours may not be recognized by the state licensing board.
If qualified clinicians are willing to take up the task without risking burnout, then handling clinical supervision in-house might be a good option – but it might not be the right answer for every facility operating under the same umbrella.
Virtual clinical supervision began to become more widely used during the pandemic shutdown.
Since 2020, almost all states began allowing 100% of supervision to be obtained virtually.
The benefits of virtual supervision:
Diversity of clinical supervisors who work with a variety of client populations and clinical specialty areas.
The ability to work with employers who operate in multiple states or have employees with multiple licenses.
Ability to more easily create dyad and group supervision cohorts.
A reduction in supervision cancellations and no-shows.
Fight the Behavioral Health Worker Shortage on Your Own Turf
When employers decide not to employ pre-licensed clinicians, they’re limiting the potential workforce that is available to local communities.
The lack of available jobs for pre-licensed clinicians hinders their ability to earn the hours they need to become licensed. With few opportunities, they often leave the profession in search of gainful employment.
And yet, an alarming number of positions remain unfilled and patients wait months for care.
When one organization decides to open up its recruitment options, it increases their ability to fill those positions, patients move off waitlists, and pre-licensed therapists get the hours and experience they need to become licensed.
When a multitude of employers take that step, many thousands of pre-licensed therapists gain the opportunity to become licensed and flourish in their chosen profession.
If employers make it a part of their behavioral health mission to provide new graduates with the work they need to move forward, the behavioral health worker shortage will lose some of its magnitude. The benefits for everyone will be both immediate and long-lasting.
Work cited
- Top Issues Confronting Hospitals. (2023). ACHE.org. (link)
- Understanding the U.S. Behavioral Health Workforce Shortage. (2023). http://commonwealthfund.org. (link)
- American Psychological Association (2023). Psychologists reaching their limits as patients present with worsening symptoms year after year. (link)
- Spies, D. (2023, February). Behavioral Health’s Impact on the Emergency Department. Beckershospitalreview.com. (link)
- SAMHSA. (n.d.). 2020 National Survey on Drug Use and Health (tables). (link)
- McCrickard, R. (2023). The Mental Health Therapist Shortage Starts at Graduation: How to Help the 57% that Never Attain Licensure. (link)
- Duffy, B and Lerner B(2023). Charting new paths: navigating the landscape of integrated behavioral health innovation. Behavioral Health Tech Conference. (link)
- Walsh, L. M., Roddy, M. K., Scott, K., Lewis, C. C., & Jensen-Doss, A. (2018). A meta-analysis of the effect of therapist experience on outcomes for clients with internalizing disorders. Psychotherapy Research, 29(7), 846–859. (link)
- Erekson, D., et al., (2017). A longitudinal study of the impact of psychological training: Does training improve client outcomes? Journal of Counseling Psychology, 64(5), 514-524. (link)
- Chow, D. L., Miller, S. D., Seidel, J. A., Kane, R. T., Thornton, J. A., & Andrews, W. P. (2015). The role of deliberate practice in the development of highly effective psychotherapists. Psychotherapy, 52(3), 337–345. (link)
- Budge, S. L., Owen, J. J., Kopta, S. M., Minami, T., Hanson, M. R., & Hirsch, G. (2013). Differences among trainees in client outcomes associated with the phase model of change. Psychotherapy, 50(2), 150–157. (link)
- Goldberg SB, Hoyt WT, Nissen-Lie HA, Nielsen SL, & Wampold BE (2016). Unpacking the therapist effect: Impact of treatment length differs for high and low-performing therapists. Psychotherapy Research, 48, 1–13. (link)
- The Hidden Benefits of Working With Pre-Licensed Therapists. (2023). Psychology Today. (link)
- Hairston, S. (2022, March). The Surprising Benefits of Seeing a Less Experienced Therapist. OpenCounseling. (link)
- Werrbach, M. (2019). Pros and Cons of Adding Provisionally-Licensed Therapists to Your Group Practice. TherapyNotes. (link)
- Adams, D. R., Williams, N. J., Becker-Haimes, E. M., Skriner, L., Shaffer, L., DeWitt, K., Neimark, G., Jones, D. T., & Beidas, R. S. (2019). Therapist Financial Strain and Turnover: Interactions with System-Level Implementation of Evidence-Based Practices. Administration and Policy in Mental Health and Mental Health Services Research, 46(6), 713–723. (link)
Support your team’s clinical development and open up your worker pool to associate counselors without burning out your staff.